

The Health Direction Bias
Why “more is better” and “less is worse” feel so safe - and how that can mislead you.

There is a habit of reasoning that can trick you about your health because it feels like common sense.
It’s the same subtle factor that resulted in a surprising increase in lung and prostate cancer in randomized controlled trials of high-dose antioxidant supplements.
I think of it as the direction bias - the habit of extending a true effect beyond its tested range.
Here’s what it looks like in practice. You learn that a certain nutrient, behavior, or metric is “good.” For example, you learn that Vitamin D is important for immune function (among other things). You may hear that people who have particularly low levels may be advised by their healthcare provider to take a supplement. From this, you intuit a general direction: more Vitamin D is better.
Or, you learn that something is “bad” - inflammation, sugar, sedentary time - and the direction locks in the other way: less is better. From that point forward, the direction itself becomes a strategy. More protein. More antioxidants. Less sun exposure. Less inflammation.
If you’re reading this letter, there’s a good chance you are not hoodwinked by most health marketing. You probably don’t buy detox teas or “immune boosting” gummies. But I’d bet that the direction bias still runs somewhere in the background of your thinking.
And the logic feels sound: if a direction is good, then more movement in that direction should be even better. What makes this deceptive is that it is often true - up to a point.
The problem is that biology is full of curves that bend. I will provide two important examples further down.
Why it persists in smart, careful thinkers
This bias exploits diligence.
The people most susceptible to the direction bias are often the ones paying the most attention to their health. They’ve read research summaries. They track their own metrics. They make deliberate choices about what they eat, how they train, and what they supplement (or don’t). That attentiveness creates a specific vulnerability: once you’ve identified a direction that is supported by evidence, the responsible choice, it seems, is to keep going.
But the evidence that established the direction almost never tested its extremes. The study that showed “X is beneficial” usually really showed that X is beneficial at a particular dose, in a particular population, over a particular timeframe, for a particular outcome. It did not show that unlimited movement in that direction produces unlimited benefit.

Most biological systems are not linear. They are shaped more like curves, where benefit increases up to a point, flattens, or sometimes reverses. Pharmacologists have a term for this general concept: the dose-response curve.
The direction is only part of the story. The shape of the curve tells the rest.
Let me show you two cases where the direction was real, the logic was reasonable, and the curve bends anyway.
The antioxidant reversal
Few health narratives have ever felt as compelling as the antioxidant story.
The reasoning was simple and, on its face, persuasive: oxidative stress damages cells, free radicals contribute to that damage, and antioxidants neutralize free radicals, so more antioxidants should mean less damage to your cells and therefore less risk of cancer.
This was biologically plausible. And, early observational data supported it - people who ate more antioxidant-rich fruits and vegetables had lower cancer rates. By the 1990s, enthusiasm was high enough that several large randomized trials were launched to test antioxidant supplements for cancer risk reduction, to confirm what many researchers and clinicians already believed to be settled science.
However, the results were not what anyone expected.
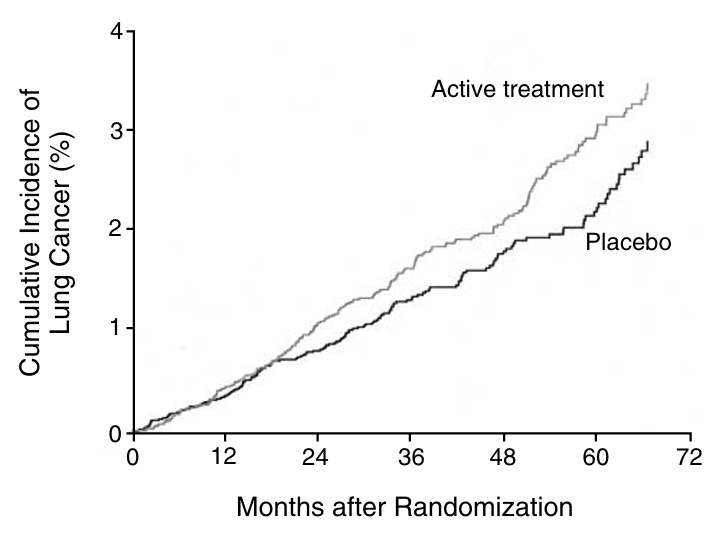
The Beta-Carotene and Retinol Efficacy Trial (CARET) enrolled over 18,000 participants at high risk for lung cancer - smokers and asbestos-exposed workers – into a randomized, double-blind, placebo-controlled study. Half of them received daily supplements of beta-carotene and vitamin A, which were anticipated to reduce risk of cancer and death through complementary antioxidant and immunologic protective effects.
However, the trial was stopped 21 months ahead of schedule at an interim data review, because participants taking the antioxidant supplements had a 28% increase in lung cancer incidence and a 17% increase in overall mortality compared to placebo.
Yikes.
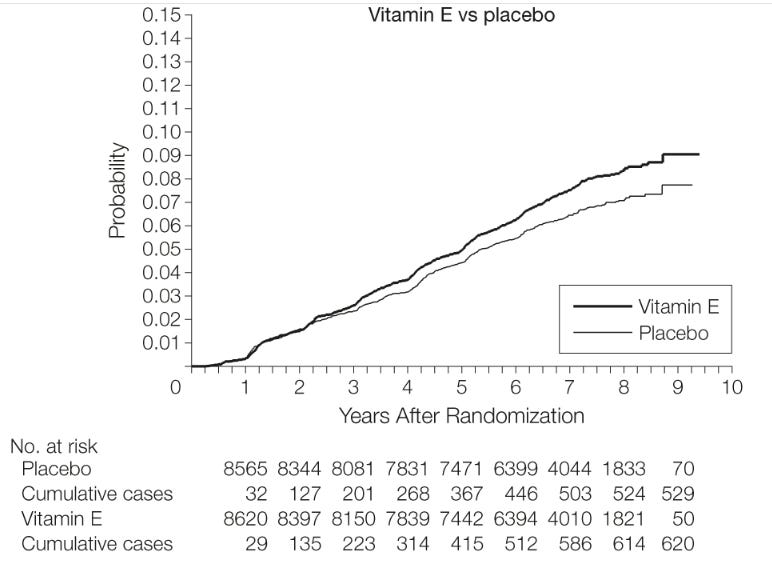
Later, the Selenium and Vitamin E Cancer Prevention Trial (SELECT) - with over 35,000 men - found that vitamin E supplementation significantly increased the risk of prostate cancer by 17%.
Yikes again.
At this point you may wonder - wait, so are antioxidants actually dangerous? No (not always). A large dose-response meta-analysis of prospective studies (Aune et al., 2018) found that higher dietary intake and blood concentrations of antioxidants like vitamin C and carotenoids from whole food sources were associated with reduced risk of cardiovascular disease, cancer, and all-cause mortality. In other words, if you eat more whole, plant-based foods rich in antioxidants, resulting in higher antioxidant levels in your body, your risk of many major diseases goes down.
But when the same compounds were isolated into supplements and given at higher dosages, the curve bent for people at risk of lung or prostate cancer. Note that these effects were observed in specific high-risk populations receiving high-dose supplementation, and the findings may have been different in other groups.
One leading hypothesis for why this could happen in these groups points out that free radicals serve dual roles in the body - they contribute to cellular damage, but they also function as signaling molecules in immune function, cell regulation, and apoptosis, the process by which the body identifies and eliminates damaged or precancerous cells. The addition of supplemental antioxidants may have interfered with some of those processes in unexpected ways.
The U.S. Preventive Services Task Force now recommends against the use of beta-carotene and vitamin E supplements for cancer or cardiovascular disease prevention.
The mechanism that made the direction feel so intuitive was real, and the direction itself was supported by a lot of evidence - over the early part of the curve. The assumption that extending it further would help even more is where things went wrong.
There is something worth pausing on here, because this is where the direction bias differs from ordinary misinformation. With many health myths, the original premise is wrong - the claim was never supported, and the error is in believing it at all. The direction bias is harder to catch precisely because the original premise is right. The early evidence for antioxidants was genuine. The biological mechanism was sound. The people who followed this direction were doing exactly what a rational, evidence-informed person would do. The mistake only emerged at the boundary, in the assumption that a relationship which held over one range of the curve must hold over all of it.
That’s the version of this problem that is most relevant to your life: the health decisions where you are most informed are the ones where you are least likely to question whether you’ve gone too far - perhaps enough to reach the bend.
The exercise paradox
Exercise is one of the most consistently supported health behaviors in modern medicine. Across decades of epidemiology, randomized trials, and mechanistic physiology, regular physical activity is associated with lower cardiovascular risk, better metabolic health, improved mood, and longer life.
If any direction in health feels earned, it’s “more physical activity = better”.
And, in almost every case, that direction holds up.
A pooled analysis published in JAMA Internal Medicine followed more than 600,000 adults and examined how different volumes of leisure-time physical activity related to death rates over time. Compared with people who were inactive, those who did any physical activity (but less than the minimum guideline of 150 minutes per week, or 7.5-15 MET h/week) had a 20% reduced risk of death (a hazard ratio of 0.80). For getting the recommended 7.5-15 MET h/week, they had roughly a 31 percent lower risk of death (HR 0.69).
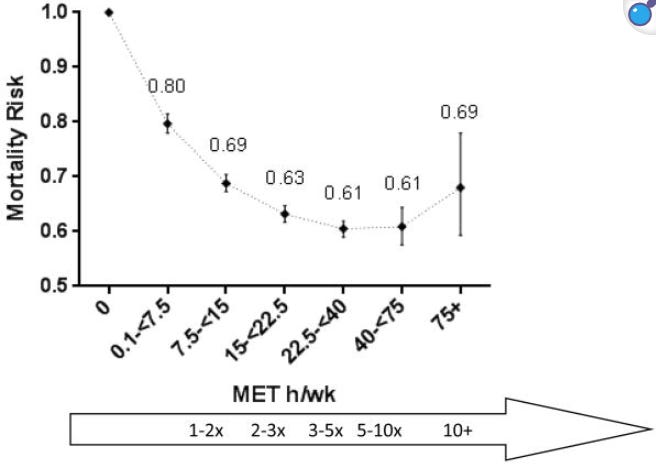
At the very high end of physical activity, even people reporting ten times the minimum recommended level (≥75 MET hours per week, or ~1,500 minutes of moderate physical activity) did not show increased mortality relative to sedentary individuals.
Importantly, even though it looks like it bends up, the mortality rate in that extreme group in this study was not statistically different from the 2nd highest group - the 40–75 MET hour category. The number of participants at those very high volumes was very small, which means wider confidence intervals and greater variability.
In other words, the data at the far right edge of the curve may visually appear to have jumped upwards in risk, but it’s unclear whether there is true evidence of harm. I think of this more as a plateau in benefits, with more statistical noise from small sample size at the extreme. In any event, unless you’re exercising in the range of 1,500+ minutes per week of moderate activity, you should be looking at a different portion of the curve!
The point is simply that physical activity yields diminishing incremental benefit at very high volumes.
There is, however, one place where a curve provides a more dramatic illustration of why the shape matters.
A systematic review and meta-analysis in the British Journal of Sports Medicine found that long-term endurance athletes had 2.46x higher risk of developing atrial fibrillation compared with non-athlete controls. The proposed mechanisms include structural remodeling of the atria after years of sustained high cardiac output, with enlargement and fibrosis that can promote irregular electrical signaling. These data primarily come from long-term endurance athletes logging very high cumulative aerobic training volumes over many years. They do not reflect the risk profile of someone performing high-intensity interval training or strength-based workouts several days per week for general fitness.
Even that finding does not erase the overall survival benefit of being highly active compared to being sedentary. Elite athletes live longer than the general population, with 27% lower rates of cardiovascular mortality and 40% reduced rates of cancer. But it does show that even for one of the most evidence-backed recommendations in medicine, specific outcomes can behave differently at the extremes.
The lesson is that, even for exercise, the curve has a shape.
Where the direction bias is simply true
It would be a mistake to walk away from this letter thinking that every health direction eventually reverses, or that “nothing is ever straightforward.” That kind of overcorrection is its own trap, and it leads to a paralysis that helps no one.
Some curves genuinely don’t bend.
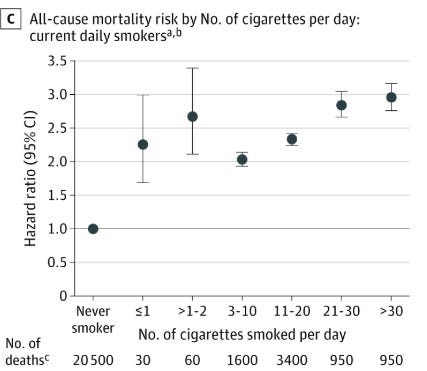
Smoking is one example. There is no J-curve. There is no beneficial range. There is no threshold below which cigarette consumption becomes neutral, compared to not smoking. Zero smoking is simply the optimal amount of smoking, from a health standpoint.
Even light or occasional smoking carries measurably elevated cardiovascular and cancer risk relative to never smoking. The relationship between smoking and harm is, as far as the evidence shows, monotonic for major outcomes like cardiovascular disease and cancer; the direction is the whole story, all the way down to zero.
The question worth keeping
When you encounter a health behavior, supplement, or recommendation where the direction feels obvious - more is better, less is worse - try adding one question to your thinking:
Does this curve bend? Where?
That question keeps you from extending a real finding beyond the range where it was actually tested, without requiring you to become cynical or to challenge everything reflexively.
A lot of good health thinking starts with a real direction, one that is grounded in evidence and worth following. The error is in the assumption that the direction never changes slope.
The most well-informed version of yourself is the one who keeps asking about the shape of the curve even after the direction has already been established, because, as the story of antioxidants and lung cancer goes to show, that is precisely where some surprisingly consequential mistakes can be found hiding.
Best,
Morgan
Morgan McSweeney, PhD (@dr.noc)
A note to my Paid subscribers: Thank you for your support of this work. Paid subscriptions allow me to keep this work independent and deeply researched. They fund research time, fact-checking, and the slower thinking that doesn’t always survive on social platforms. If you’ve found value in this newsletter, a paid subscription is the most direct way to strengthen my work here and elsewhere.
Great article! In the 90s I was the PI on a study looking at the impact of vitamin e on NKC activity to inhibit leukemia cell growth.
Preliminary in vitro results were exciting! But when we started dosing monkeys with the levels we thought would drive enhanced cancer surveillance something weird happened. Plasma levels plateaued well below the targeted levels seen to enhance NKC activity.
The problem was that vitamin e was sequestering in fat and liver cells resulting in toxicity before any measurable increase in NKC activity happened.
The study came to an abrupt end.
Many thanks! Very informative with great examples. It made me think of Paracelsus's "Only the dose makes the poison." Except smoking, of course!